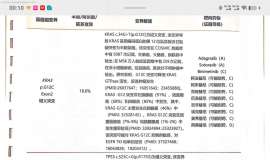
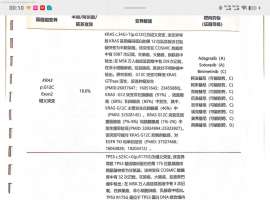
非小细胞肺癌中的PTEN突变及其与EGFR、ERBB2、KRAS和TP53突变的关系
7 r& f) ~3 R0 O. }( tPTEN mutations and relationship to EGFR, ERBB2, KRAS, and TP53 mutations in non-small cell lung cancers , V! ?$ d$ s1 D1 |
作者:Jin G, Kim MJ, Jeon H-S, Choi JE, Kim DS, Lee EB, 4 o* Y) V" M: U! _3 H
期刊: 《LUNG CANCER》2010年9月3期69卷
% w7 W9 c% N2 I# O$ s
2 T; u% R( V) m. I! JSomatic mutations of phosphatase and tensin homolog deleted on chromosome ten (PTEN) in non-small cell lung cancers (NSCLCs) have been investigated in but a small number of cases. In addition, the relationship between PTEN mutations and epidermal growth factor receptor (EGFR), KRAS, and TP53 mutations has not been investigated. Therefore, we investigated the frequency of PTEN mutations in 176 surgically resected NSCLCs and analyzed the relationship between PTEN mutations and EGFR, ERBB2, KRAS, and TP53 mutations. Mutations of PTEN (exons 1-9), EGFR (exons 18-21), ERBB2 (exons 19 and 20), KRAS (exon 1), and TP53 (exons 2-11) were determined by polymerase chain reaction and direct sequencing. PTEN mutations were present in 8 (4.5%) of the 176 tumors. PTEN mutations were only found in ever-smokers and were significantly more frequent in squamous cell carcinoma than in adenocarcinoma (10.2% vs 1.7%, P= 0.02). Mutations of EGFR, ERBB2, KRAS, and TP53 genes were found in 36 (20.5%), 2 (1.1%), 11 (6.3%), and 66 (37.5%) cases, respectively. Of the 8 tumors with PTEN mutations, 1 case concurrently had an EGFR mutation and 4 cases had TP53 mutations. However, PTEN mutations were not found in the tumors with KRAS mutation. Our findings indicate that PTEN mutations are relatively common in NSCLC, and thus analysis of PTEN mutations may facilitate a comprehensive understanding of the genetic alterations related to the EGFR signaling pathway.% j( k( ]4 J- D& S$ s4 b) h
|
 肺腺癌晚期ⅣB,基因靶点KARS-G12C,
各位老师,我哥肺腺癌晚期,患有强直性脊柱炎,目前治疗方案为:贝伐单抗+化疗药,10
肺腺癌晚期ⅣB,基因靶点KARS-G12C,
各位老师,我哥肺腺癌晚期,患有强直性脊柱炎,目前治疗方案为:贝伐单抗+化疗药,10
 发现招募:转移性结直肠癌(mCRC)患
招募:转移性结直肠癌(mCRC)患者
地点:山西医科大学第一医院肿瘤消化科
研究主
发现招募:转移性结直肠癌(mCRC)患
招募:转移性结直肠癌(mCRC)患者
地点:山西医科大学第一医院肿瘤消化科
研究主
 肝硬化肝腹水,失代偿,求助哪里医生
家人查出肝硬化肝腹水,年轻时有乙肝,一直状况良好,未治疗,今年由于劳累,感觉没劲
肝硬化肝腹水,失代偿,求助哪里医生
家人查出肝硬化肝腹水,年轻时有乙肝,一直状况良好,未治疗,今年由于劳累,感觉没劲
 BRCA突变患者迎来高质量长生存,助力
作者:Tony
从2018年第一个PARP抑制剂在我国上市,到如今,想找到一个在临床上还没用
BRCA突变患者迎来高质量长生存,助力
作者:Tony
从2018年第一个PARP抑制剂在我国上市,到如今,想找到一个在临床上还没用
 KRAS G12D: 安罗替尼+曲美替尼?
各位朋友请教一下:
基因检测靶点KRAS G12D, 目前单用安罗替尼,但安罗替尼有耐药迹
KRAS G12D: 安罗替尼+曲美替尼?
各位朋友请教一下:
基因检测靶点KRAS G12D, 目前单用安罗替尼,但安罗替尼有耐药迹






 显身卡
显身卡 $ S; F ^) G0 v
$ S; F ^) G0 v